Contraception Options For Trans Guys
Trigger warning - this article discusses body parts using anatomical terms (medical words).
Finding the right contraception can be difficult, especially when you are on (or planning on starting) testosterone. There are lots of options, and many pros and cons to consider. This article will break down the choices. It is not individual medical advice, so please talk to your doctor about what might be right for you. Remember that condoms are the only form of contraception that also protects against STIs.
Testosterone is not contraception.
While T can reduce your fertility, it is not reliable contraception. It suppresses ovulation (egg being released from the ovary), but this effect can be unpredictable. If pregnancy occurs while you’re on T, the medicine can be harmful to the developing fetus. That’s why anyone having front-hole sex with a partner assigned male at birth should use contraception.
This is still true even if your partner is on oestrogen.
Progesterone versus Oestrogen
The two main ingredients in hormonal contraception are progesterone and oestrogen. Some contraceptives use both hormones (so-called “combined contraception”) and some only use progesterone (“progesterone-only”). Many trans guys want to avoid taking oestrogen, so this article focuses on the progesterone only methods. I have included some information on the combined methods and non-hormonal options towards the end.
The Implant - Implanon NXT

What: a match-stick sized implant
Where: Placed under the skin near the biceps muscle
How: Very minor surgical procedure
When: Can stay in for three years (and be removed at any time)
Why: Very effective (>99.9%), does not require any intimate examination, discrete
Why not: About 30% of people have annoying irregular or constant spotting (although this is much less likely if you’re on T and already avoiding periods. Acne can become worse (T does this too) and some people notice weight and mood changes.
The IUD - Mirena or Kyleena

What: small T-shaped devices - the Mirena (4.4mm wide when inserted) and the Kyleena (3.8mm wide when inserted)
Where: Placed inside the uterus
How: Performed during a procedure similar to a “pap smear” or pelvic / speculum exam. This requires an intimate examination that can cause some people dysphoria. For more detailed info, see my article on What to expect during an IUD insertion.
When: Kyleena - lasts 5 years. Mirena - lasts 8 years.
Why: Localised action and very little hormone enters the bloodstream (compared with other methods that need to travel through the blood to have an effect), very effective (>99.9%), long-lasting, great at stopping any ongoing bleeding while on T
Why not: Intimate examination can worsen dysphoria, the procedure can be anything from uncomfortable to very painful
The thought of an IUD insertion can be a big barrier for some people. Here’s how I can help to make it a safer experience.
Trauma informed approach - regular check-ins. You are the boss and in control the entire time! If you say, “Stop”, I stop, no questions asked. Rests, breaks and time-outs are totally fine.
No surprises - I provide a careful explanation throughout the entire procedure.
Atrophy - T can cause genital dryness, which makes the procedure more uncomfortable. I prescribe some cream to use for 1-2 weeks before the procedure to help.
Anxiety - I help with distraction and relaxation techniques, but some people need medication like diazepam.
Pain - I discuss all the options for pain relief prior to the procedure, so you can choose what sounds best for you. This can include simple over the counter pain relievers, stronger opioid medicine, the green whistle (Methoxyflurane), or nerve-blocking injections around the cervix.
Going under - if the thought of an IUD insertion still sounds like too much, we can discuss a referral to have the procedure done under general anaesthetic.
The Pill - Slinda
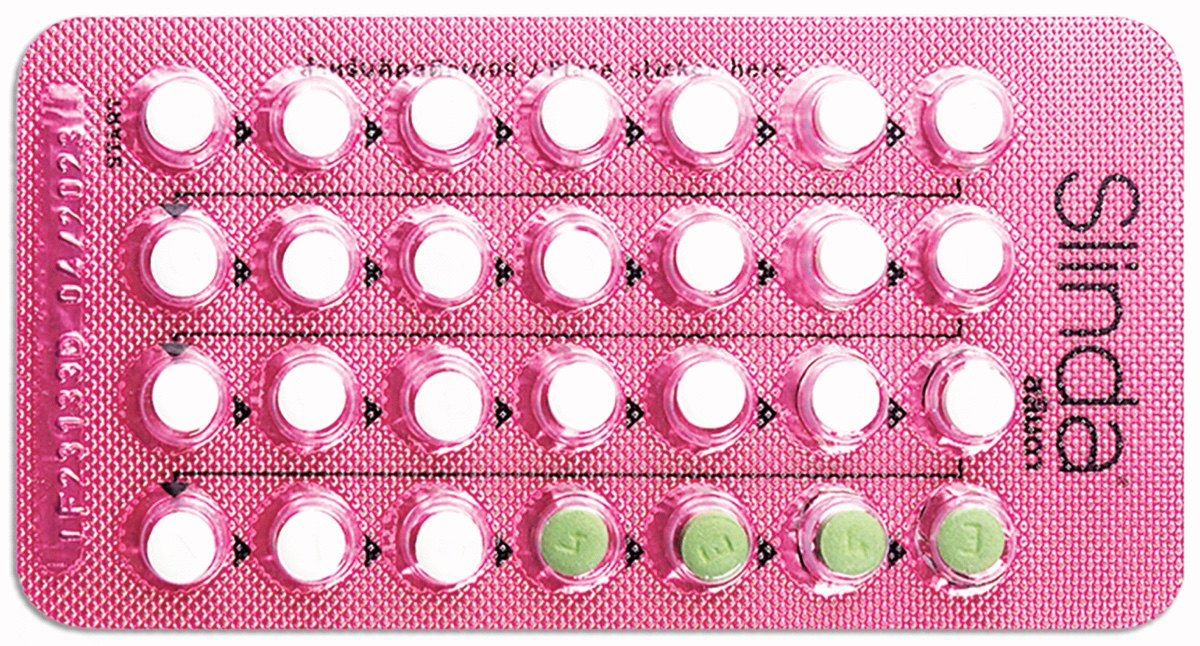
A progesterone-only pill. It is a new medication that is more reliable than older "mini-pill" progesterone only medication.
How: taken daily (you might be advised to take the white active pills continuously and skip the sugar pills).
Why: taking a pill may be easier than a procedure or implant. Slinda is usually quite good at stopping periods. If you forget to take a pill, you are still protected as long as you take your pill within 24 hours from when your last pill was due.
Why not: you need to remember to take the pill every day, and forgetting increases the risk of pregnancy. Irregular bleeding is a possible side effect (though is less common while on testosterone). The active ingredient in Slinda is technically an anti-androgen, meaning it could theoretically slow down the effects of testosterone. However, it is a low dose pill and many people still achieve their goals on testosterone and Slinda. Like any systemic hormone, possible side effects include mood changes, weight changes and chest tenderness.
Alternatives: If a pill is right for you, but you don't want to take an anti-androgen, you could consider older progesterone-only pills (like levonorgestrel), however they are not as effective at stopping a pregnancy.
The Shot - Depo provera
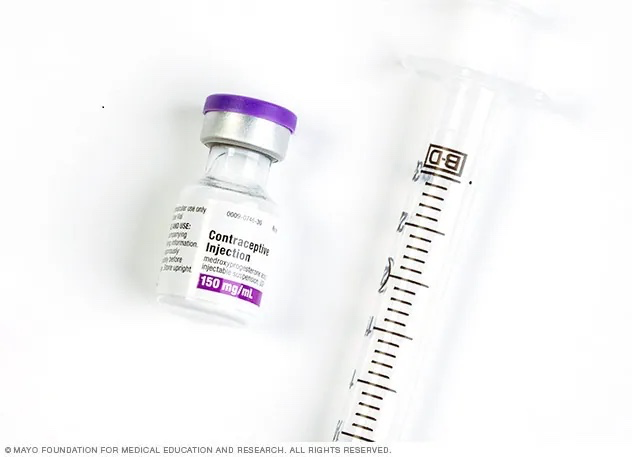
What: an injection that prevents pregnancy
How: given by a doctor or nurse
When: every 12 weeks
Where: the shot is usually given in the arm or the buttock muscle
Why: reliable and effective. Can be timed well with a Reandron (testosterone) injection! It is private (no pill packets required).
Why not: Some folks find it hard to commit to a doctors appointment every 3 months. Long term use can lead to thin bones (reduced bone density, or osteoporosis). There may also be other side effects that come along with systemic hormones to consider (weight gain, mood changes, chest tenderness). If you plan on pausing your transition to carry a pregnancy in the future, it can take 6-12 months for your cycle to return after stopping the shot.
Combined Options (pill, ring)
Combined pills

Combined hormonal pills contain both oestrogen and progesterone. While they're highly effective at preventing pregnancy, they come with some specific considerations for trans guys:
Many different types are available, with varying doses and formulations
Oestrogen may cause chest tenderness and swelling, which can worsen dysphoria
Could reduce the effect of testosterone, and slow down your transition
Increased risk of blood clotting, particularly if you're over 35 or smoke
May require regular check-ins with your doctor to monitor for side effects
Ring
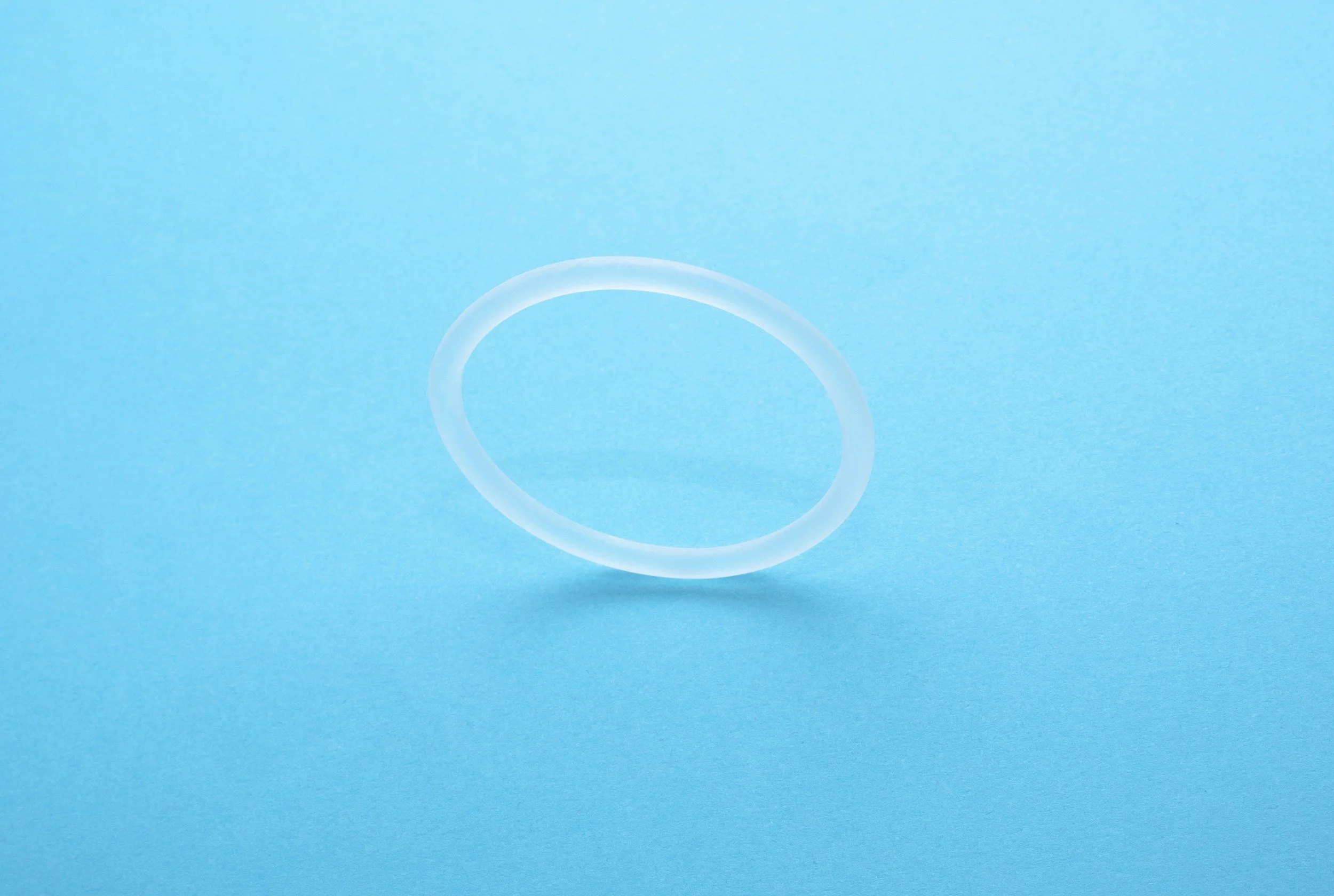
The vaginal ring is a flexible plastic ring that releases hormones similar to the combined pill:
A ring inserted into the front hole, and kept in place for 21 days out of every 28-day cycle
Dysphoria with frequent insertions can be a significant barrier for some people
Same hormones enter the bloodstream as the combined pill, so similar considerations apply
Some people find it more convenient than remembering a daily pill
Like the combined pill, it may interfere with testosterone effects
Non-hormonal methods
Barrier methods (internal and external condoms)

Barrier methods are the only contraceptive options that also protect against sexually transmitted infections (STIs).
External condoms are widely available and easy to use
Internal condoms (also called female condoms) are inserted into the front hole before sex
Both may sometimes fall off or break, and aren't as effective as other methods at preventing pregnancy
Require consistent use with every act of penetrative sex
Can be combined with other methods for increased effectiveness
Copper IUD
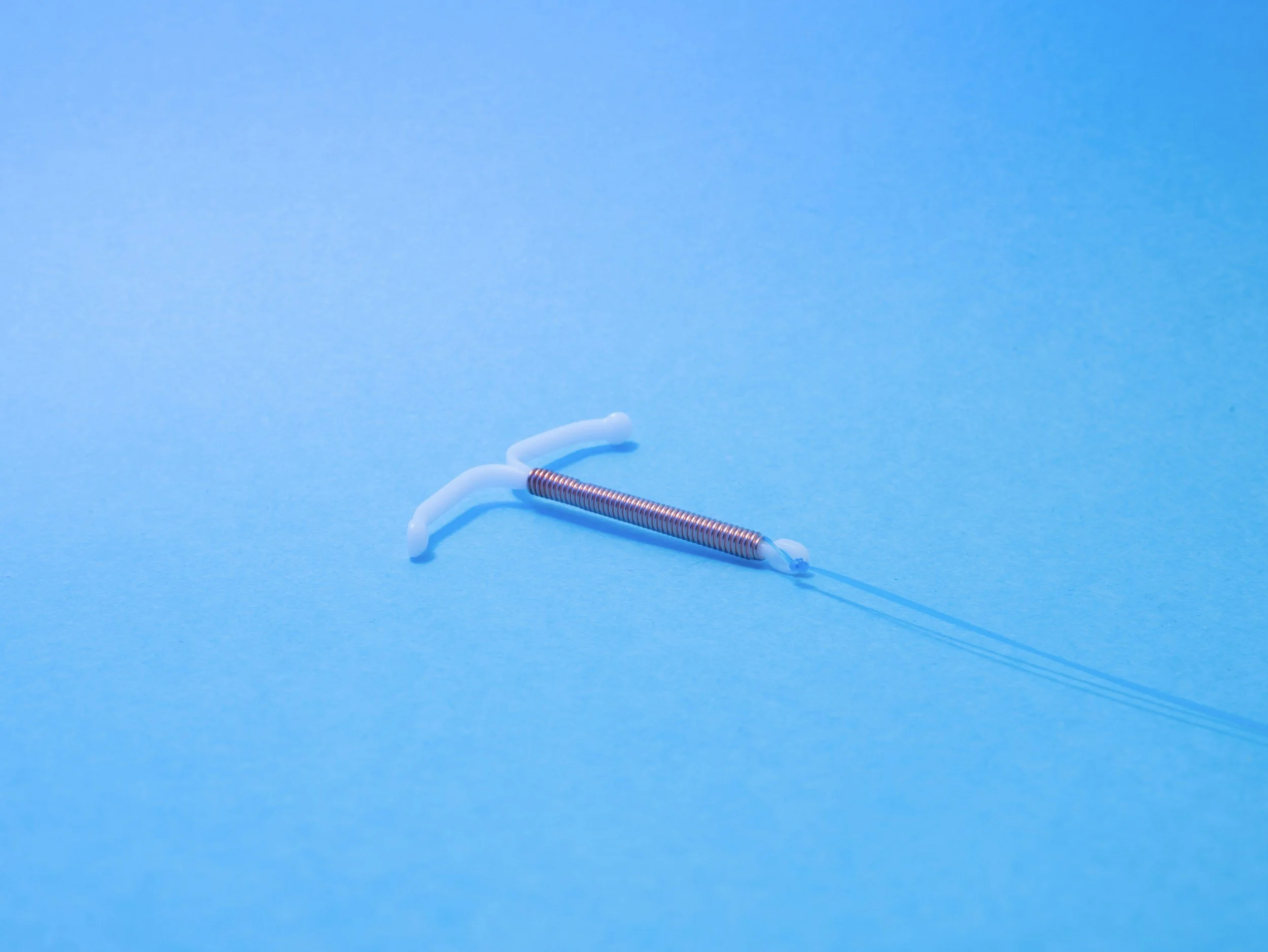
The copper IUD is a non-hormonal option that works differently from hormonal methods:
Very effective at preventing pregnancy (>99.9%), with no hormones involved
Works by being toxic to sperm cells, preventing fertilisation
Can increase menstrual bleeding and cramping, which may be a concern if you're not on testosterone
Lasts 5-10 years depending on the type
Requires the same insertion procedure as hormonal IUDs, which can cause dysphoria
A good option if you want to avoid all hormones while still having long-acting protection
Pull-out method (withdrawal)
The pull-out method is not a reliable form of contraception and is not recommended as a primary method of birth control. Pre-ejaculate can contain sperm, and timing is difficult to get right consistently.
Conclusion
Choosing the right contraception is a personal decision that depends on your individual needs, preferences, and medical history. Whether you prioritise effectiveness, convenience, hormone-free options, or protection against STIs, there are multiple methods available to suit different situations. The most important thing is to have an open conversation with a healthcare provider who understands your needs and can help you weigh the pros and cons of each option. Remember that testosterone is not reliable contraception on its own, and that condoms remain the only method that protects against both pregnancy and STIs. Whatever you choose, the goal is to find a solution that allows you to feel safe, while supporting your transition and overall wellbeing.